


Lung Cancer
About one fourth of all people with lung cancer have no symptoms when the cancer is diagnosed. These cancers are usually identified incidentally when a chest X-ray is performed for another reason. The other three-fourths of people develop some symptoms. The symptoms are due to direct effects of the primary tumor; to effects of cancer spread to other parts of the body (metastases); or to disturbances of hormones, blood, or other systems.

Symptoms of lung cancer include cough, coughing up blood or rusty-colored phlegm, fatigue, unexplained weight loss, recurrent respiratory infections, hoarseness, new wheezing, and shortness of breath.
- A new cough in a smoker or a former smoker should raise concern for lung cancer.
- A cough that does not go away or gets worse over time should be evaluated by a health care provider.
- Coughing up blood (hemoptysis) occurs in a significant number of people who have lung cancer. Any amount of coughed-up bloodshould be evaluated by a health care provider.
- Pain in the chest area is a symptom in about one fourth of people with lung cancer. The pain is dull, aching, and persistent.
- Shortness of breath usually results from a blockage in part of the lung, collection of fluid around the lung (pleural effusion), or the spread of tumor through the lungs.
- Wheezing or hoarseness may signal blockage or inflammation in thelungs that may go along with cancer.
- Repeated respiratory infections, such as bronchitis or pneumonia, can be a sign of lung cancer.
Symptoms of metastatic cancer depend on the extent and location of the cancer spread.
- Lung cancer most often spreads to the liver, the bones, and the brain.
- Metastatic lung cancer in the liver may cause yellowing of the skinand eyes (jaundice), but it may not cause any noticeable symptoms at the time of diagnosis.
- Lung cancer that has metastasized to the bone causes bone pain, usually in the bones of the spine (vertebrae), the thigh bones, and the ribs.
- Lung cancer that spreads to the brain can cause difficulties with headaches, vision, weakness on one side of the body, and/orseizures.
Paraneoplastic syndromes are the remote, indirect effects of cancer not related to direct invasion. Symptoms include the following:
- New bone formation (particularly in the fingertips) that can be painful
- High levels of calcium in the blood
- Blood clots
- Low sodium levels in the blood
What are the types of lung cancer?
Lung cancers, also known as bronchogenic carcinomas (“carcinoma” is another term for cancer), are broadly classified into two types: small cell lung cancers (SCLC) and non-small cell lung cancers (NSCLC). This classification is based upon the microscopic appearance of the tumor cells. These two types of cancers grow, spread, and are treated in different ways, so a distinction between these two types is important.
SCLC comprises about 10%-15% of lung cancers. This type of lung cancer is the most aggressive and rapidly growing of all the types. SCLC is strongly related to cigarette smoking. SCLCs metastasize rapidly to many sites within the body and are most often discovered after they have spread extensively.
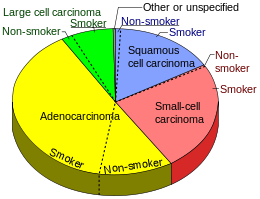
NSCLC is the most common lung cancer, accounting for about 85% of all cases. NSCLC has three main types designated by the type of cells found in the tumor. They are:
- Adenocarcinomas are the most common type of NSCLC in the U.S. and comprise up to 40% of lung cancer cases. While adenocarcinomas are associated with smoking like other lung cancers, this type is also seen in non-smokers — especially women — who develop lung cancer. Most adenocarcinomas arise in the outer, or peripheral, areas of the lungs. They also have a tendency to spread to the lymph nodes and beyond. Adenocarcinoma in situ (previously called bronchioloalveolar carcinoma) is a subtype of adenocarcinoma that frequently develops at multiple sites in the lungs and spreads along the preexisting alveolar walls. It may also look like pneumonia on a chest X-ray. It is increasing in frequency and is more common in women. People with this type of lung cancer tend to have a better prognosis than those with other types of lung cancer.
- Squamous cell carcinomas were formerly more common than adenocarcinomas; today, they account for about 25% to 30% of all lung cancer cases. Also known as epidermoid carcinomas, squamous cell cancers arise most frequently in the central chest area in the bronchi. This type of lung cancer most often stays within the lung, spreads to lymph nodes, and grows quite large, forming a cavity.
- Large cell carcinomas, sometimes referred to as undifferentiated carcinomas, are the least common type of NSCLC, accounting for 10%-15% of all lung cancers. This type of cancer has a high tendency to spread to the lymph nodes and distant sites.
Lung Cancer Treatment options overview
- About one-third of lung cancer patients are diagnosed with localized disease that may be treated by either surgical resection or, if the patient is not a candidate for full surgical resection, with definitive radiotherapy. Another third of patients have disease that has already spread to the lymph nodes. In these cases, radiation therapy along with chemotherapy and occasionally surgery is used. The last third of patients may have tumors that have already spread to other parts of the body via the blood stream and are typically treated with chemotherapy and sometimes with radiation therapy for the relief of symptoms.
- Surgery with removal of the entire lobe in which the tumor is located, is the primary treatment for patients with early-stage cancer who are in good general health. The goal of surgery is to totally eliminate all the tumor cells and thereby provide a cure. Unfortunately, lung cancers tend to develop in smokers more than 50 years of age, who very often have other lung disease or serious medical conditions that magnify the risk of surgery. The location and size of a lung tumor dictate how extensive the operation must be. Open thoracotomy or less invasive video-assisted thoracic surgery, using smaller incisions, may be recommended for appropriately selected patients.
- Lobectomy — removal of an entire lobe of the lung — is an accepted procedure for removing lung cancer when the lungs are functioning well. The mortality risk is 3 percent to 4 percent, and tends to be highest in older patients. If lung function prohibits lobectomy, a small cancer confined to a limited area can be removed with a small portion of surrounding lung tissue. This is called a sublobar resection, and may be either a wedge resection or a segmentectomy. There is a possible higher risk of recurrence with more limited surgery than a lobectomy. Sublobar resections cause less loss of lung function, as a smaller portion of lung is removed, and carries an operative mortality risk of 1.4 percent. If the entire lung must be taken out by pneumonectomy, the expected mortality rate is five to eight percent. The oldest patients are at highest risk and recurrent cancer is very common. In a majority of cases, either the patient is not fit for surgery or it is not possible to remove the entire tumor because of its size or location.
- Radiofrequency ablation (RFA) and microwave ablation (MWA) use image guidance to place a needle through the skin into a tumor within the chest. In RFA, high-frequency electrical currents are passed through an electrode, creating a small region of heat. In MWA, microwaves are created from the needle to create a small region of heat. The heat destroys the lung cancer cells. RFA and MWA may be used to treat lung tumors or provide palliative care. They are effective treatment options for patients who might have difficulty with surgery and for those for whom surgery is not an option due to the spread of a tumor to the lungs from the primary tumor or cancers outside the chest.
- Radiation therapy, or radiotherapy, delivers high-energy X-Ray that can destroy rapidly dividing cancer cells. It has many uses in lung cancer:
- As primary treatment
- Before surgery to shrink the tumor
- After surgery to eliminate any cancer cells that remain in the treated area
- To treat lung cancer that has spread to the brain or other areas of the body
How does the treatment method depend on the type of lung cancer?
There are two main types of lung cancer that have different microscopic appearances:
- Small-cell lung cancer (SCLC)—also referred to as oat-cell cancer—usually is found in active or former cigarette smokers. Although SCLC is less common than the other type of lung cancer, it is a more aggressive tumor that is more likely to spread to other body sites. Chemotherapy is the mainstay of the treatment for SCLC. Radiation therapy is often used along with chemotherapy to treat lung tumors that have not spread beyond the chest or other organs. Surgery is not commonly used in SCLC due to its tendency to spread quickly. While surgery is seldom used to treat patients with SCLC, occasionally it is used to obtain tissue samples for microscopic study to determine the type of lung cancer present. For small cell lung cancer, after treatment directed to the disease in the chest, the radiation oncologist may suggest radiation therapy directed at the brain even though no cancer has been found there. This is called prophylactic cranial irradiation and is given to prevent lung cancer metastases from forming at this vital site.
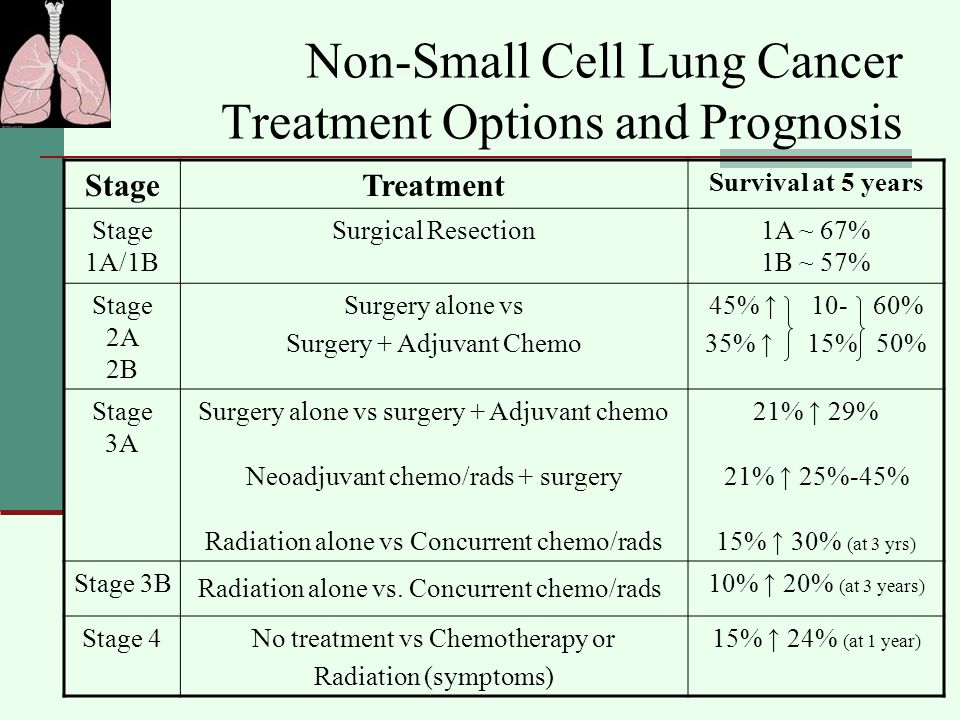
- Non-small-cell lung cancer (NSCLC) tends to grow more slowly and takes longer to spread beyond the lung. Local treatments such as surgery and/or radiation therapy are the main-stay of treatment for NSCLC. If chemotherapy is used, it is often to increase the effectiveness of surgery or chemotherapy, and is generally different in NSCLC than in SCLC. Different types of chemotherapy may be used for different types of non-small cell lung cancer.
Contact us and get Second Opinion from Expert Oncologists at your preferred city.
You can also reach out to us contact@expertchikitsa.com


{kind=link}